
Oral Myofunctional Therapy Helps Improve Sleep Apnea
Oral Muscle Function Training
Hello everyone, I'm Dr. Emma! Today I want to share with you an exercise that can help many people, and that is "Oral and Pharyngeal Muscle Function Training." This is actually the underlying principle behind the "MRC trainers" that many children wear, or the "mewing" techniques that many internet influencers share to make the face look smaller. Why do we need to train the oral and pharyngeal muscles? Simply because there are so many benefits!
Oral Myofunctional Therapy focuses on exercising the muscles used for chewing, swallowing, and the airway. The goal is to strengthen the muscles of the oropharynx. It helps maintain the tongue in its correct position in the mouth, preventing muscle compensation issues that arise from weakness or incorrect use, such as reverse swallowing and tongue thrust.

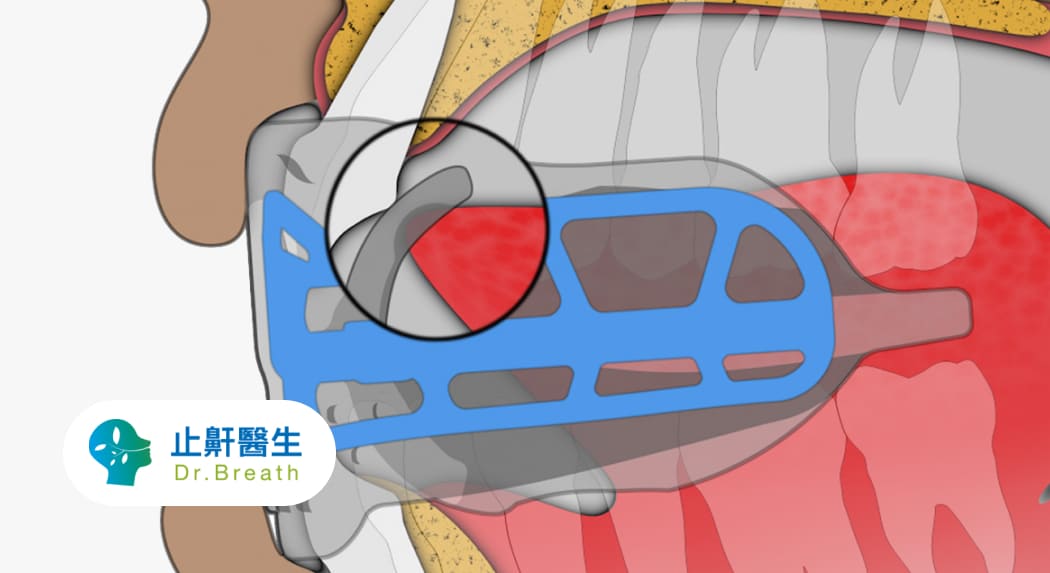
Image: A too-small oral cavity (retrognathic lower jaw and dentition) restricts the tongue, leaving it with no room, making it look as if the tongue is overflowing. Both sides of the tongue have teeth marks, and it occupies the airway space in the throat backward, so the airway located in the throat cannot be seen.
The oropharynx is the airway in the throat behind the oral cavity. It is a soft tube made of a mucosal lining and muscles. These muscles help us eat, speak, and breathe. They also help keep the airway open, especially during sleep.
When the muscles of the oropharynx are weak, they can disrupt airflow, which can lead to snoring. If they allow the tube to collapse, the airway becomes blocked, which is what happens during sleep apnea. Furthermore, a weak and floppy tongue may fall back into the throat and cause an obstruction.
Oral Myofunctional Therapy aims to strengthen the muscles of the oropharynx and the tongue. It helps to maintain the tongue in its correct position in the mouth.
The Origins of Oral Myofunctional Therapy
The origins of oral myofunctional therapy can be traced back to 1882 when George Catlin wrote the book "Shut Your Mouth and Save Your Life." George Catlin observed the living habits of Native Americans for a long time and found that due to their beliefs, they considered opening the mouth to attract bad luck. Therefore, they specifically required their infants to develop the habit of keeping their mouths closed. This prolonged mouth-closing action strengthened the orbicularis oris muscle group.
Additionally, the Native American diet mainly consisted of whole foods with fewer modern refined processed foods. Thus, when chewing food, stronger oral muscle use was required. These lifestyle habits indirectly and significantly lowered the rate of mouth breathing among Native Americans, allowing the upper and lower dental arches to develop fully and resulting in fewer cases of crowded teeth. By learning from the experiences of Native Americans, we understand that oral myofunctional training can indeed improve our lives.
How to Train Oral Muscles?
Oral myofunctional training is akin to going to the gym to train your chest muscles, biceps, etc. Its purpose is to increase muscle elasticity and reduce the chances of muscle weakness. So, how do you train?
There are four steps in sequence:
-
Breathing
Take two deep breaths, then exhale all the air and start holding your breath. When you are about to run out of breath, place your hand over your lips and deliberately feel yourself breathing through your nose. The goal is to learn the correct method of nasal breathing. This training is extremely important for children, as it can prevent the developmental obstruction of the jawbone, which in turn affects the width of the airway.
-
Tongue
There are many ways to train the tongue muscles. Here is one of the simplest and easiest methods to start with. Place the tip of your tongue at the junction of the upper front teeth and the upper palate, and slide it back and forth along the upper palate. Repeat this exercise continuously to stimulate the tongue to generate an upward force. This helps ensure that the tongue has enough muscle strength during sleep to rest against the upper front teeth, preventing the base of the tongue from falling backward and thereby compressing or obstructing the airway.
-
Swallowing
The correct way to swallow is with the tongue pressed against the upper palate. Facial muscles should not be used when swallowing; the patient should rely solely on the strength of the tongue muscles to complete the swallow. The most common incorrect swallowing methods involve shrugging shoulders, nodding, or blinking during the swallow.
-
Lips
Finally, there is the training of the orbicularis oris muscle around the lips. The training method is to first take a breath and then tightly close your lips. At this point, continuously push the air in your mouth forward, imagining that you are trying to push the air out of your mouth. Conversely, your lips must remain tightly closed to prevent the air from leaking out. The purpose of this training is to increase the strength of the orbicularis oris muscle around the mouth so that our lips can close naturally when in a relaxed state. This significantly reduces the incidence of mouth breathing.
The Effects of Oral Myofunctional Therapy
According to a 2020 Meta-Analysis report, oral myofunctional therapy alone can significantly improve sleep apnea. The research report shows that oral myofunctional training can:
- Significantly reduce daytime fatigue and improve concentration (the quantitative index for daytime sleepiness dropped from 5.47 to 0.53).
- The snoring intensity index also dropped from a severe level (> 50 db) to a mild level (40~45 db).
- The most astonishing result was a significant drop in the AHI index, which decreased from an average of about 18 to about 8, equivalent to a reduction of 10 sleep apnea events per hour.
Furthermore, children can use oral myofunctional training to correct the bad habit of mouth breathing. Long-term mouth breathing will hinder the growth of the jawbone (commonly known as a small chin). Besides affecting teeth alignment and bite, a receding chin will also cause the problem of a narrow airway, and the longer-term impact is the development of sleep apnea.
Start with simple oral myofunctional training to improve sleep apnea.
What is Sleep Apnea (OSA)?
Sleep Apnea (OSA) refers to the partial or complete closure of the upper airway during sleep. The human body is unable to effectively expel air with a high carbon dioxide concentration and exchange it with outside air that has a higher oxygen content. This causes the blood oxygen saturation level in the body to drop, leading to the need for more labored breathing to raise the blood oxygen level, ultimately affecting sleep quality.
Generally speaking, sleep apnea can be divided into two categories:
Obstructive Sleep Apnea
In obstructive patients, the chest and lung functions operate normally (rising and falling), but air exchange with the outside is difficult due to airway obstruction. This type of patient is mainly affected by physiological structures or muscle function degeneration. For example, long-term mouth breathing affects jawbone development, ultimately affecting the airway radius.
Excessive obesity causes fat to accumulate in the muscles and tissues of the airway, reducing the airway radius. Or, the weakness of the airway dilator muscles and tongue muscles causes the base of the tongue to retreat and the soft palate to collapse, thereby causing airway obstruction. Symptoms in this type of patient can be improved through physical therapy.
Central Sleep Apnea
Central patients are affected by the central nervous system, and their chest and lung functions cannot operate normally, leading to sleep apnea. This type of patient cannot be effectively treated using physical methods.
How to Determine the Severity of Sleep Apnea?
Apnea-Hypopnea Index / AHI
The severity of symptoms is determined by the number of apneas or hypopneas that occur per hour during sleep. The criteria are as follows:
- Normal: AHI < 5
- Mild: 5 < AHI < 15
- Moderate: 15 < AHI < 30
- Severe: AHI > 30
Epworth Sleepiness Scale (ESS)
Assesses daytime sleepiness. A higher score represents a higher degree of sleepiness.
Snoring Intensity
Determined by the volume (decibels) of the snoring sound.
- Mild: 1 (40~45 db)
- Moderate: 2 (45~55 db)
- Severe: 3 (55~60 db)
- Very Severe: (>60 db)
How to Treat Sleep Apnea?
Currently, the most common treatment for sleep apnea is wearing a "Continuous Positive Airway Pressure (CPAP)" machine.
CPAP Machine (Continuous Positive Airway Pressure)
The CPAP machine uses a pressure difference to pump outside air with high oxygen content into the patient's airway, directly and efficiently solving the problem of low blood oxygen concentration in the patient. When patients wear a CPAP machine, it indeed significantly lowers the AHI index and reduces the occurrence of sleep apnea.
Although CPAP machines have a significant therapeutic effect, they are difficult to carry around, and the potential discomfort of wearing an oxygen mask while sleeping reduces patients' willingness to wear them long-term. Another treatment method is to wear a "Mandibular Advancement Device" (MAD) while sleeping. Its purpose is to move our lower jawbone forward, increasing the space of the oropharyngeal airway and improving the efficiency of breathing during nighttime sleep.
Although both CPAP machines and MAD oral appliances can improve sleep apnea and lower the AHI value, the symptoms are only improved while they are being worn, requiring long-term cooperation from the patient.
Is There a Cure for Sleep Apnea?
The most intuitive and fundamental treatment method is to use surgery to directly remove the obstructing factors, for example: removing an overgrown epiglottis cartilage, or clearing circular obstructions in the airway, etc. However, most people are intimidated by surgery and seek more conservative physical therapies.
According to research, for every 10% of weight lost, the chance of sleep apnea drops by as much as six times.
Additionally, weight loss can reduce fat accumulation in the airway and effectively improve sleep apnea. Besides weight loss, promoting oral muscle group training aims to increase the function of the upper airway dilator muscles. This method is safe, has no side effects, and does not require expensive equipment fees. Furthermore, compared to weight loss, which requires long-term persistence and effort, oral myofunctional training can show noticeable results in the short term.
Conclusion
Sleep apnea is a hidden killer. General patients may not pay special attention to it, but you must know that the long-term decline in sleep quality can lead to chronic diseases such as cardiovascular disease, diabetes, etc.
Therefore, for patients who snore in the middle of the night, or experience unexplained daytime lack of focus and fatigue, if you are hesitant about surgery and dislike wearing a ventilator or MAD oral appliance at night, why not start with simple oral myofunctional training to improve this symptom that everyone often ignores but can cause many chronic diseases in the long run?
References
Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea (Review)
Atilgan E, Kunter E, Algun ZC. Are oropharyngeal exercises effective in Obstructive Sleep Apnea Syndrome? J Back Musculoskelet Rehabil. 2020;33(2):209-216. doi: 10.3233/BMR-171101. PMID: 31282395.
The content is based on the professional experience of physicians. Results may vary depending on individual conditions. Please consult a healthcare professional for personalized medical advice.